Supraventricular Tachycardia
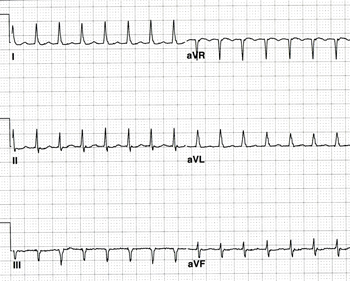
Supraventricular tachycardia (SVT) includes atrial tachycardia and a group of disorders known as paroxysmal supraventricular tachycardia (PSVT). Paroxysmal supraventricular tachycardia is characterized by a rapid, regular, narrow QRS complex arrhythmia with sudden onset and termination. The most common variety of PSVT arises from the AV nodal complex and is known as AV Nodal Reentry Tachycardia (AVNRT). This is responsible for most PSVT in adults. The rate can vary between 120 and 220 beats per minute. At faster rates, a rate-related bundle branch block may result in widening of the QRS complex. In the most common form of AVNRT, P-waves are not visible on the surface ECG since they are buried in the QRS complex. Hence, the older term for this rhythm disturbance was “junctional tachycardia.” AVNRT occurs because of reentry over the slow and fast AV nodal pathways (transitional fibers) and so it does not originate from within the AV node. The AV node is part of the circuit, however, which is why this arrhythmia can be terminated abruptly by intravenous AV nodal blocking agents such as adenosine, diltiazem, verapamil, and beta blockers. There are several varieties of AVNRT. “Common” AVNRT (seen above) is caused by a reentry wavefront that travels down the slow pathway and back up the fast pathway. This is also known as “slow-fast” AVNRT. Uncommon AVNRT is referred to as “fast-slow” AVNRT. As can be deduced from the name, the antegrade limb is the fast pathway and the retrograde pathway is the slow pathway. A third form of AVNRT known as “slow-slow” can occur in a small number of patients who have multiple slow pathways.
Patients who have AVNRT can often terminate the tachycardia by increasing vagal tone with the Valsalva maneuver or carotid massage. On occasion, sustained tachycardia will result in an emergency room visit. IV adenosine or diltiazem are very effective in terminating this tachycardia since they both cause transient AV block that stops the circus movement. Adenosine works within seconds and can be over 95% effective if administered properly. Long-term pharmacologic therapy aimed at slowing AV node conduction (such as beta blockers, verapamil, or diltiazem) can reduce the frequency and severity of attacks. However, these medications are often ineffective, they frequently result in significant side effects, and they may be pro-arrhythmic (the arrhythmia can occur more frequently, albeit at a slower and perhaps more tolerable rate). Catheter ablation of the slow AV nodal pathway can permanently eliminate the arrhythmia in over 95% of patients with only a 1-2% risk of complete AV block requiring a permanent pacemaker. Catheter ablation is the treatment of choice in most symptomatic patients, particularly young patients who would prefer to avoid long-term medical therapy.
The second most common type of PSVT is known as AV Reentry Tachycardia or AV Reciprocating Tachycardia (AVRT). AVRT results from reentry caused by an accessory AV pathway, which is an extra electrical connection between the atria and the ventricles. In some patients, the accessory pathway is capable of conducting the electrical signal in an antegrade direction (from the atria to the ventricles), bypassing the AV node. This deforms the QRS complex in a characteristic manner, resulting in a short PR, a wide QRS, and a slurred onset of the QRS (known as a “delta wave”) with secondary ST/T wave abnormalities. This pattern of pre-excitation is diagnostic of the Wolff-Parkinson-White (WPW) Syndrome. A premature atrial or ventricular beat can act as a "trigger" to initiate AVRT. Most often, reentry occurs down the AV node, thorough the ventricular myocardium, up the accessory pathway, and back to the atrial myocardium, where it is free to go down the AV node again, thus completing the circuit. This is known as “orthodromic” AVRT and results in a narrow QRS tachycardia with retrograde P-waves (inverted in leads II, III, and aVF) that begin just after each QRS complex. The tachycardia behaves like AVNRT in that it is rapid and regular, with sudden onset and termination. In young patients it may occur at rates up to 240 beats per minute. Rarely, "antidromic" AVRT occurs due to reentry down the accessory pathway and back up the AV node (or up a second accessory pathway). This results in a wide QRS complex because conduction down the accessory pathway causes “maximal pre-excitation.”
Many patients with orthodromic AVRT do not exhibit the classic findings of WPW Syndrome on their ECG because these patients have a “concealed” accessory pathway that is only capable of retrograde conduction. These concealed accessory pathways can still cause orthodromic AVRT. Thus, all patients with AVRT have an accessory pathway (concealed or overt), and AVRT is responsible for up to 25% of PSVT in adults and the majority of PSVT in children. Patients with overt WPW Syndrome can also develop atrial fibrillation with very rapid conduction (approaching 300 beats per minute) down the accessory pathway. This arrhythmia can result in ventricular fibrillation. Patients with WPW and rapid conduction of atrial fibrillation down the accessory pathway appear to be at increased risk of sudden death. A significant portion of young children and adults who die suddenly while playing competitive sports do so because of this condition.
The acute treatment of sustained AVRT is the same as AVNRT. Since the AV node is part of the circuit, AVRT will usually terminate with intravenous adenosine or diltiazem. To prevent recurrent episodes, AV nodal blocking agents can be used. In addition, other potent antiarrhythmic agents have been used to affect conduction in the accessory pathway (which is sodium-dependent). Atrial fibrillation with rapid conduction down an accessory pathway in a patient with WPW Syndrome should never be treated with verapamil, since this can actually increase the rate of conduction down to the ventricles and may result in ventricular fibrillation. Although medical therapy can be used to treat AVRT, the treatment of choice is catheter ablation of the accessory pathway. This procedure is over 95% successful at permanently eliminating the problem with only a 1-2% risk of serious complications. Catheter ablation is preferable to long-term medical therapy in most patients. Catheter ablation should be performed in patients with recurrent symptomatic PSVT, patients with WPW and rapidly conducting accessory pathways, and in asymptomatic patients with WPW who are in a position of responsibility (e.g. airplane pilot, bus driver), where the occurrence of symptoms could place others in jeopardy.